
Yes, they usually heal faster.
While investigating breast enhancement, any patient comes across the heated debate of location at least once: Sub-Muscular (Under the Muscle) or Sub-Glandular (Over the Muscle). Oftentimes your plastic surgeon will make this decision look like the most suitable for your body’s features but people still tend to lean towards the option “Over the Muscle” for one very specific and appealing reason: the promise of a super-fast and almost painless recovery.
Some may have heard the narrative about the “weekend recovery” or seen over-the-muscle friends washing their hair right after surgery while under-the-muscle ones were limping for a week. The simple response to the query is yes, Over-the-Muscle implants indeed can heal significantly faster and with less pain however, in the field of plastic surgery, the memorably euphoric, ‘free lunch’ doesn’t exist. The recovery that is “easy” comes with certain aesthetic compromises that one has to discern well before making a trade of pace first, structure last. We at Lin Europe Clinic, consider that although the first week of recovery is important, the next ten years of results carry more weight. Below is an extensive explanation of why the recovery is so different and whether or not the “easy way” suits you.
Why Does Muscle Bring More Pain: The Anatomy of It

What made us look at the line up of recovery, was the amount of body trauma done by the surgery.
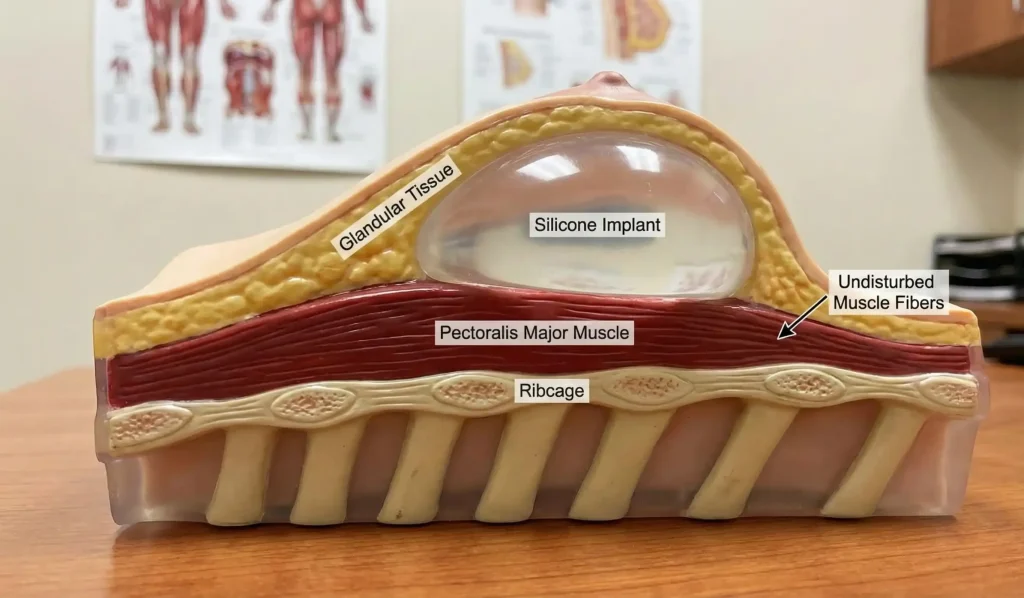
- Sub-Glandular (Over): The surgeon work on an area next to the breast tissue but above the chest muscle. This is a dissection of “soft tissue”. The muscle is kept as it is, not touched and figuratively still asleep.
- Sub-Muscular (Under): In order to make a space for the implant under the muscle, the surgeon had to release the attachments of the pectoralis major muscle and show the ribs.
Since the over-the-muscle approach does not tear up the muscle fibers, the patient does not get the painful cramping muscle spasms which are the main discomfort after the sub-muscular procedure. Generally over-the-muscle patients have their discomfort described as a “heavy soreness” or “pressure” which they compare to a feeling of a breast engorgement during breastfeeding. On the contrary, sub-muscular patients usually explain a feeling of “an elephant sitting on the chest” or unbearable tightness which does not allow even full breathing in the first 2-3 days. Therefore, patients with over-the-muscle implants discontinue their use of narcotics a few days earlier than those with under-the-muscle implants.
The “T-Rex Arms” Is Only Funny Until It Happens
The “T-Rex arms” phase, a widely known breast augmentation feature, signals the time when patients can only just barely raise their arms. This is pretty much a Sub-Muscular problem running most of the show. Pectoral muscles being the Prime Movers of the arms means that as you get that glass of water or try to brush your hair, the pain comes from the muscle getting injured each time you do a movement which will really limits the things you can do.
With an Over-the-Muscle solution, your arm motions are hardly limited. Since the muscle is not divided, raising your arms, washing your hair, and dressing yourself can usually be done without any problem within 24 to 48 hours. Your independence is returned to you as if it was never lost. Mothers who work with their kids all day or women with physically demanding jobs will give functional freedom a massive scale of merit. You may not be a “disabled” person, you just have a “skin wound” in the process of healing.
The “Drop and Fluff” Shortcut
We usually advise the patients to wait on their implants to “Drop and Fluff” (settle into the pocket and round out) for 3 to 6 months, which is a very different story when it comes to over-the-muscle implants whose timeline is incredibly shortened.
When implants are dipped under a tight muscle, that muscle is like a strap holding the implant high and flat against the chest wall. The muscle has to loosen up, which can take weeks or months, for the implant to be allowed to “drop”.
In Over-the-Muscle placement, there is no muscle strap holding the implant up. Therefore, the force of gravity is the main one and it acts immediately. Hence, it will be a matter of weeks before you can see your implants nice and round, full and well positioned. In fact, you miss out on the “square breast” or “torpedo” period almost completely and get to enjoy your final looks earlier.
The Trade-Off: Why Isn’t Everyone Doing It?
If the pace of recovery is made faster, the level of pain during healing is lowered and the result is ready to be observed sooner, then why does the surgeon community essentially and without exception stick to Under-the-Muscle (Dual Plane) for most patients? The real answer is in the soft tissue coverage.
The muscle layer adds an important extra layer of padding to the implant’s top.
- The Rippling Risk: If muscle is not present, then the only thing on top of the implant is the skin and natural breast fat. Being thin will almost certainly lead to you witnessing and feeling your implant’s border (rippling) in the cleavage area. The implant may look like a “ball under the skin” rather than a natural slope.
- Capsular Contracture: Over-the-muscle breast implants have historically been associated with a slightly higher rate of Capsular Contracture (scar tissue hardening). The continual infection from microbes present in the milk ducts and the absence of regular muscle massage are thought to be responsible for the risk of breast hardness in the long term.
- The Sag Factor: Inside, the muscle is acting as a bra helping to hold the implant’s weight being transferred against the chest wall. The over-the-muscle implants have their entire dependency on the skin’s elasticity to keep them in position. The longer the time goes by, the more gravity gains, and thus these implants are more likely to sag (bottom out) sooner than the ones supported by muscle.
Who is the Perfect Match for Over-the-Muscle Technique?
Over-the-muscle placement, however, is the better choice for a very limited group of women: Professional Athletes and Bodybuilders.
If your job or hobby involves substantial chest muscle usage (CrossFit, bodybuilding, tennis, pole fitness) putting an implant under the muscle will most probably bring the problem of Animation Deformity—the implant is visibly distorted or it moves sideways when one flexes. For these particular women, the “easy recovery” is only a bonus, the functional goal is really separate breast aesthetics from muscle function. It also works perfectly for ladies who have a sufficient natural breast tissue (pinchable fat) to cover up the implant edges thus giving them the best of both worlds: easy recovery and natural results.
Frequently Asked Questions About Implant Placement Recovery
The answer is yes, a subglandular placement is much less painful since it does not involve cutting or stretching the pectoral muscle, the major source of deep pain after breast augmentation.
Usually, you may start to do lower-body exercises and light cardio after 2 weeks, and upper-body workout after 4 weeks, which is quite a bit quicker than the 6-8 week recovery period for submuscular implants.
Yes, when the implant is only supported by the skin and glandular tissue without the muscle acting as an internal support, the effect of gravity is greater, and hence the implant is pulled down quicker leading to sagging earlier than normal.
For very thin patients, it is generally discouraged as there would be almost certain visible rippling and palpable implant edges in the upper pole if the implant is not cushioned by the muscle layer.
Bodybuilders pick this location to avoid “Animation Deformity” which happens if the pectoral muscles are flexed during a competition, resulting in the implant visibly distorting, flattening, or jumping sideways.
Code, T. (2000). Subglandular versus subpectoral breast augmentation: A study of complications and patient satisfaction. Aesthetic Plastic Surgery.
Brown, M. H., et al. (2005). Cohesive silicone gel breast implants in aesthetic and reconstructive breast surgery. Plastic and Reconstructive Surgery.
Spear, S. L., & Baker, J. L. (2012). Animation deformity in the subpectoral breast augmentation patient. Aesthetic Surgery Journal.




