
It is a collapsed nasal bridge after surgery.
Septoplasty is in principle a functional nose surgery that does not impact the nose externally but is aimed at straightening the deviated septum and improving the patient’s breathing. A few patients notice an unbearable aesthetic change in their profile weeks or months after the operation: the bridge of your nose dips in, creating a hollowness like the nose of a boxer. A saddle nose deformity is the medical term for such a nose pattern. It is the consequence of the collapse of the middle part of the nose, which results not only in the deformation of the nose but also, ironically, in a worsening of the breathing problems that the surgery was originally intended to relieve.
A procedure that was supposed to be a quick fix of a medical problem turns into a real nightmare psychologically for the patient. The nose looks wider when seen from the front and has an odd “ski-slope” profile when seen from the side. At Lin Health Europe Clinic, we are trained for the complicated reconstruction that is necessary for fixing such a deformity. We are aware that it is not just about vanity; it is about restoring the architectural integrity of your face and your ability to breathe freely. Familiarizing oneself with the reasons for such a collapse is a prerequisite to having faith in the surgeon who will be entrusted to restore it.
The Anatomy of Collapse: The “L-Strut” Concept
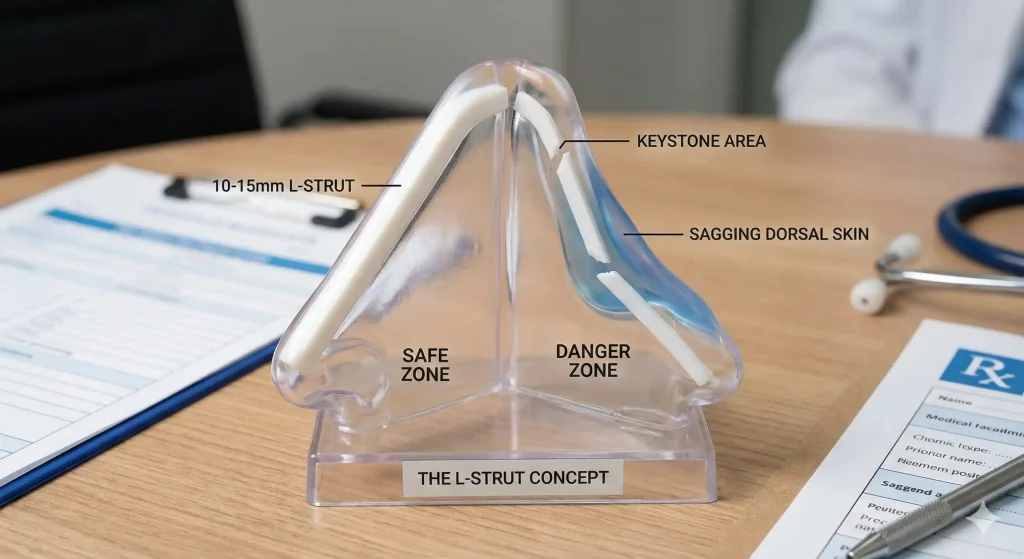
Therefore, it is very important to emphasize that the septum is not just a wall separating the two nostrils but also a tent pole supporting the roof. The most important part of the septum is this L-shaped piece of cartilage that runs along the bridge and down the front of the nose. It is known as the L-Strut. The surgeon is advised to keep at least 10 to 15 millimeters of this cartilage during septoplasty to allow the nose to resist opposing forces such as gravity and scar contraction.
When the L-strut suffers a breach, the deformity of a saddle nose occurs. This problem arises when the surgeon, in an attempt to remove the deviated cartilage, becomes overly daring and opens up the airway by over-resecting the area. The remaining portion will be too thin or weak and will buckle like a pillar under the loads. Hence, the crushing of the weakened cartilage is due to the weight of the nose and the force of the contracting scar tissue; this results in the middle vault of the nose deforming. This is practically never the patient’s fault; it is simply a structural failure during the surgery.
Functional Consequences: The Valve Collapse
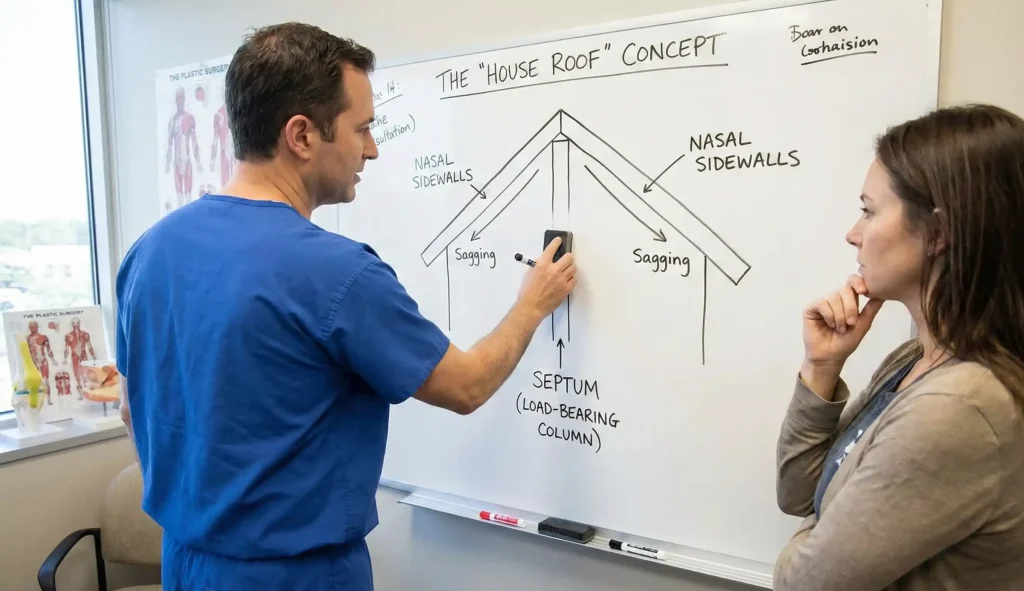
The deformity that can be seen with the naked eye is by far the most prominent indication of the problem. Yet, the functional deterioration might even be greater. In fact, the internal nasal valve, which is the narrowest part of the airway, depends on the height of the septum to be kept open. The lowering of the septum causes the roof of the nose to drop in, thus significantly narrowing this valve. Therefore, this situation may be considered as a paradox as the patient can feel more blocked after the surgery than before, although the aim was exactly the opposite.
Saddle nose deformity sufferers report that it is hard for them to describe their obstruction sensations but if they breathe in, they can feel the air flow but it is uneven or restricted coming in. They also may have experiences of “valve collapse” which refers to the sensation of the nostrils shutting each time the patient attempts to inhale deeply. Because the mucosal lining inside the nose is getting folded up when the nasal support structure drops, the following problems might occur – chronic crusting, bleeding, and whistling sounds. Hence, medically it is a necessity to reestablish the height of the nose to reopen the airway and restore laminar airflow.
The Reconstruction: Why We Need Ribs
First of all, repairing a saddle nose deformity is much more complicated than a primary nose job as it is basically a work on a subtraction. Merely stitching up the wound is not enough, a missing supporting pillar has to be built. Because the septal cartilage has already been removed or damaged, the nose is merely a “bare shelf.” Consequently, for us to restore the height and the profile, strong material capable of providing structural support must be brought in from a different part of the body.
That is to say, saddle nose revision almost inevitably calls for a Costal Cartilage Graft (Rib Graft). The shape, softness, and flexibility of ear cartilage are such that they would not provide proper support for the nasal bridge. Thus, one might say that if the house is made out of rubber, it is impossible to build a solid structure. On the contrary, rib cartilage is hardly ever curved, is very plentiful, and is quite hard. To be more specific, at Lin Health Europe Clinic, we take a tiny portion of your rib from which we shape a “Dorsal Onlay Graft” that fills the saddle hollow and a “Septal Extension Graft” that restores the tip’s strength, thus both these elements are combined at the same time. This autologous way is far better than using synthetic materials such as silicone, which are prone to extrusion (coming through the skin) very easily especially when placed under the thinned and scarred skin of a saddle nose.
Camouflage vs. Cure: The Limits of Filler
Many patients, scared by the possibility of undergoing another operation, choose to use dermal fillers or “Liquid Rhinoplasty” to cover up the flaw. Indeed, a Sessile Acid injection into the depression can temporarily mask this kind of deformity thus making the profile appear straight once again. This will be a pretty good solution for very mild cases or for patients who are not fit for surgery due to health reasons.
Nevertheless, filler is basically a cosmetic cover-up and it is not a structural cure. It only temporarily increases volume, but it does not provide structural support. It is totally ineffective in opening the collapsed airway or in strengthening the nasal valve. Besides, injecting filler into a previously surgically treated nose poses a higher risk of vascular complications because the blood supply has been altered. Moreover, filler will diffuse over time which will, in all likelihood, cause the nose to appear wider. Only structural grafting is capable to providing a permanent and functional solution since it goes deep into and directly addresses the collapse’s main cause.
Lin Europe Clinic: Precision Preservation
At Lin Europe Clinic, we are convinced that prevention is the best medicine for a saddle nose. We use Piezo ultrasonic technology and very strict libraries while carrying out primary septoplasties. We always preserve a sturdy L-strut. We give the septum the same treatment as a supporting wall load with which we do not sacrifice stability for the sake of performing super-aggressive resections.
For those who come to us for revision, we handle the rib reconstruction with the expertise that the specific trauma of a “failed” operation demands. By way of advanced imaging, we are able to demonstrate to you how we intend to restore your bridge. We perform Structural Rhinoplasty which is based on creating a solid tripod of support that will last a lifetime. At the end of the day, not only do you get a nose that looks like it has never been broken, but it also breathes better than the one before your first procedure.
Frequently Asked Questions About Saddle Nose Deformity
Yes. While a saddle nose deformity can occur right away, more often it is a slow process that takes months or even years. The scar tissue contracts and gradually weakens the septal cartilage that is left, until finally there is collapse of the nasal bridge.
Yes. Since the bridge collapses, the internal nasal valves become narrower, thus causing severe congestion. A saddle nose deformity repair is usually necessary to get the proper airflow back.
You can hide it with dermal fillers (“liquid rhino”) but it is just a temporary solution and also you will still have the problem with breathing. Only surgical reconstruction can permanently fix a saddle nose deformity.
The nasal area itself will not be very painful, however, if a rib graft is used, the chest will be sore for a few days. For the pain during saddle nose deformity reconstruction we implement nerve blocks to be very effective.
In most cases, yes. Since a saddle nose deformity is a condition causing valve collapse resulting in airway obstruction, therefore reconstruction will be regarded as medically necessary by the majority of health insurance plans rather than only for cosmetic reasons.
Toriumi, D. M. (2006). Subtotal septal reconstruction: an update. Facial Plastic Surgery Clinics.
Tardy, M. E., et al. (1995). The over-resected nose. Facial Plastic Surgery.
Daniel, R. K. (2010). Rhinoplasty: An Atlas of Surgical Techniques. Springer.




