
Yes, breastfeeding is often still possible.
Most women who choose to undergo a breast lift (mastopexy) are probably at some stage in their life when they need to make that choice. They have got to the stage where they no longer want to accept that their breasts have become saggy due to gravity, weight loss, or simply due to genetics; on the other hand, they expect to have kids and breastfeed their babies at some point in the future. As a result, this situation causes such a worry: can the surgical fixing of the breasts aesthetically kill their biological function? What is really worrying is surgery cutting off the milk ducts to such an extent that it becomes impossible to breastfeed.
In brief, yes, you can normally breastfeed after a breast lift, if the operation is carried out with neo-techniques that keep the nipple-gland tissue connection intact. Nevertheless, there could still be some functional modifications in that scenario even if the “plumbing” is preserved. Learning about which part of the breast gets lifted and the kinds of risks involved, allows women to choose smartly whether to get a breast lift now or wait till they have their last baby.
The Anatomy of Milk: Ducts vs. Skin
You have to figure out the distinction between a breast lift and a breast reduction in order to gauge the risk. The method of breast reduction implies physically getting rid of a huge amount of gland parcels (milk production factories) from the body of the breast. However, a breast lift just purifies the skin from the defects brought forth by the loss of elasticity and reshapes the tissue thoroughly without removing the actual gland. The mammary glands are normally still there, having been left almost completely intact. Thus, all the tools needed for milk synthesis are still present.
The most important thing is the mast duct network that runs from the gland at the depth of the breast up to the nipple. Typically, the surgeon does not “hollow out” the breast when carrying out the procedure of a breast lift. This means that the rest of the ducts right behind the mammary glands remain intact and continue their function. Theoretically, some very small branches may be cut during the rearrangement of the tissues, but the process of milk secretion is so well established (and thus has a built-in redundancy) that there are numerous alternative routes through which the milk can reach the baby.
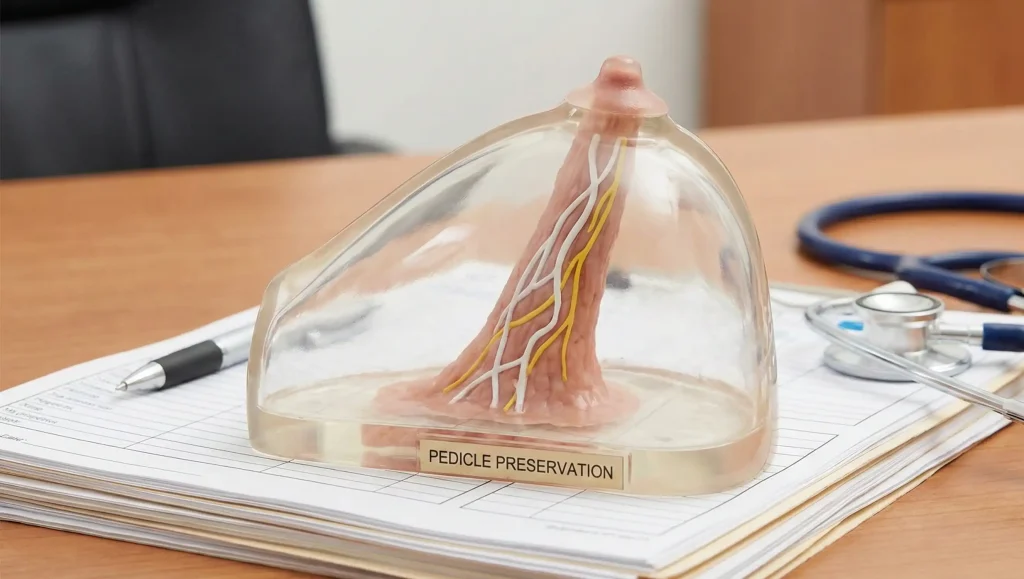
The Critical Factor: The “Pedicle” Technique
The fundamental determinant of whether you will be able to breastfeed your baby after the operation or not is probably the way the nipple was moved by surgical incision. In the present-day practice of plastic surgery, the employment of a “Pedicle” technique is almost an axiom on our part. Let us say that the nipple is the flower and the pedicle is the basket. The surgeon raises the nipple to the desired height, while at the same time, keeping it connected to a “stalk” of living tissues that contains vessels of blood, nerves, and milk ducts.
If the pedicle is not cut, then there is a blood supply to the nipple through it, and there is also a potential pathway for the milk to flow. A danger would only be if, in extreme cases the breast ptosis grade 3 is so high that, in such a condition, the use of a pedicle would be considered risky and therefore should be avoided. In such abilities, the local plastic surgeon performed the procedure called “Free Nipple Graft”, where the nipple is removed completely, cut off and then used as a graft to the breast skin. By means of this technique, all the anatomical structures, such as nerves or milk ducts are severed. Hence, it is not possible to breastfeed after the surgery. Be aware that this is an extremely rare case after a regular breast lift option and it is mainly not suitable for a big reduction.
Sensation and the Let-Down Reflex
Besides being merely mechanical, breastfeeding is also a neurological process. The baby’s sucking sends a message to the brain through the sensory nerves that release the hormone oxytocin that in turn causes the milk to be squeezed out of the alveoli. However, mama’s nipple, after the operation, can sometimes become numb due to the injury of the nerves during the surgical treatment of the nipple.
In the case of lack of sensation, the brain may not get the signal to release milk and thus breastfeeding cannot be effectively carried out even if the milk ducts are clearly open. Luckily, nowadays so-called “pedicle” techniques are commonly employed in plastic surgery making total and permanent loss of sensation something uncommon. There often is a decrease in volume or even the kind of “feeling” may change after the surgery, but most of the women still have enough sensitivity left that facilitates the let-down reflex. Yet it may take a little more time and effort for them to do the trick than it usually does for a non-operated breast.
Supply Issues: Managing Expectations

Unlike many women, some women may not be able to breastfeed at all or they may find that their breastmilk production is low. The truth of the matter is that milk production can be reduced after the breastlift. The reason could be that scar tissues formed inside the breasts, causing pressure on the milk-producing glands and thus reducing the secretion of milk. Also, some nerve injury during surgery could be the cause of reduced regulation of milk production.
That is why women who have undergone the breastlift operation are advised to be flexible about feeding their babies. They may succeed in exclusive breastfeeding or may have to use supplemented formula. This, however, is not a shortcoming but merely a biological variation. The best thing to do is to check the baby’s weight regularly, especially in the initial weeks. The fact that you had surgery does not mean that milk isn’t there but the milk production rate is slower, thus the baby has to put in more effort to get the milk.
Lin Europe Clinic: Nipple-Sparing Protocols
At Lin Europe Clinic in Turkey, we believe that your breasts are not just parts of your body that need to be treated but elements of your reproductive identity that should, therefore, be respected. One of the first questions you will be asked at your consultation will be about your plans for having children. Knowing that, we will customize our operation plans to ensure that ductal preservation is at the forefront.
We rely on techniques that use “medial” or “inferior” pedicles, and these techniques statistically yield the highest breastfeeding success rates. Besides that, we do not tighten the tissue around the areola thereby preventing the milk from flowing. Our doctors have the skills to strike a perfect balance between the risk and reward of a breast surgery that provides the patient with both a perky, young look and the possibility of being a capable mother. We guarantee that you will look great when you leave our clinic today, and you will still be able to fulfill your role as a mom tomorrow.
Frequently Asked Questions About Breast Lift and Breastfeeding
As a rule, no. Today’s breast lift operation methods generally entail the use of a “pedicle” to maintain the attachment of the nipple with the underlying gland, thus the major milk ducts from the mother’s breast remain intact for breastfeeding.
Sometimes it can. Only a few women may not get back the sensation, but most of them do. However, temporary numbness is the norm. In breastfeeding, the sensation that triggers the “let-down reflex” is essential, so if numbness remains, it will be harder to nurse after a breast lift.
Yes. An augmentation-mastopexy (implants plus a breast lift) oftentimes involves placing the implant beneath the muscle, which is quite far from the milk glands, so it is considered safe for breastfeeding.
There is definitely a risk. It is possible that some experiments rely on the logic that a decreased amount of milk comes about due to the formation of scar tissue or alterations in nerves. If you try to breastfeed after a breast lift, you might have to give some formula as a supplement.
Exactly. A breast lift might be able to cure the condition of inverted nipples by letting the nipple be free and releasing the tight tethering tissue which, actually, after this procedure breastfeeding will be easier than before the surgery.
Harris, L., et al. (2015). Breastfeeding outcomes following breast reduction and mastopexy. Plastic and Reconstructive Surgery.
O’Shea, A., et al. (2020). The impact of breast reduction and mastopexy on breastfeeding: A systematic review. Journal of Plastic, Reconstructive & Aesthetic Surgery.
Cruz-Korchin, N. (2009). Breastfeeding after vertical mammaplasty with medial pedicle. Aesthetic Plastic Surgery.




