Yes, a second breast reduction is possible.
The majority of patients consider a Breast Reduction (Reduction Mammaplasty) as a once-in-a-lifetime event. It is often hailed as the plastic surgery procedure with the highest patient satisfaction, immediately addressing and getting rid of years of back pain, shoulder grooving, and skin rashes. Nevertheless, the human body is not a fixed piece of art; it is a living, evolving organism. Some women, even years or decades after their initial surgery, may find themselves in front of the mirror, disappointed to see that their breasts appear to have “grown back,” or they simply want to be smaller than what their original surgeon dared to do.
Aesthetic medicine professionals are divided over the issue of “Can I repeat the operation?” Among the questions in aesthetic medicine, this is one of the most complicated ones. The answer in brief is: yes, a second breast reduction can be performed. Nonetheless, it is hardly a matter of just “cutting off a bit more.” A subsequent reduction is a highly technical, reconstructive procedure that comes with significantly greater risks. The anatomy has been changed, the blood supply has been rerouted, and the tissue is loaded with scar adhesions. Lin Health Europe Clinic is a center of expertise for such complicated revision cases. We uphold an uncompromising honesty about the vascular risks involved and the specific surgical compromises—such as occasionally having to resort to Free Nipple Graft—that are necessary to keep you safe while attaining the smaller, lighter figure that you deserve.
The Regrowth Biology: Why Do They Come Back?

Figuring out if a second breast reduction is feasible would be the case after we have determined the reason for the breasts being large again. In adults, true regeneration of the gland tissue that has been removed is a biologically rare occurrence, but “regrowth” is a very real phenomenon that is mainly influenced by hormonal and metabolic factors. The main reason is almost always weight gain. The composition of the breast is gland and fat. If a patient after the first surgery gains 10 to 15 kilograms, the leftover fat cells of the breast will experience hypertrophy (increase in size), thus negating the reduction. In such a situation, the “regrowth” is the expansion of fat only, and the treatment could be as simple as liposuction rather than full open surgery.
Nonetheless, the true proliferation of glands can be triggered by hormonal changes. Pregnancy is considered the strongest factor; the surge of estrogen, progesterone, and prolactin prepares the breast for milk production and results in the enlargement of the glands and skin stretching (ptosis) that may be permanent. On the other hand, menopause causes a change in the breast tissue composition where dense glands are replaced with less dense fat which can give a feeling of heaviness or sagging even though technically the volume has stayed the same level. The essence of the matter is figuring out if your relapse indicates the presence of fat, gland, or an excess of skin (bottoming out), since that will be the deciding factor in the approach to your safe second breast reduction.
Vascular Scar Tissue: An Obstinate Issue
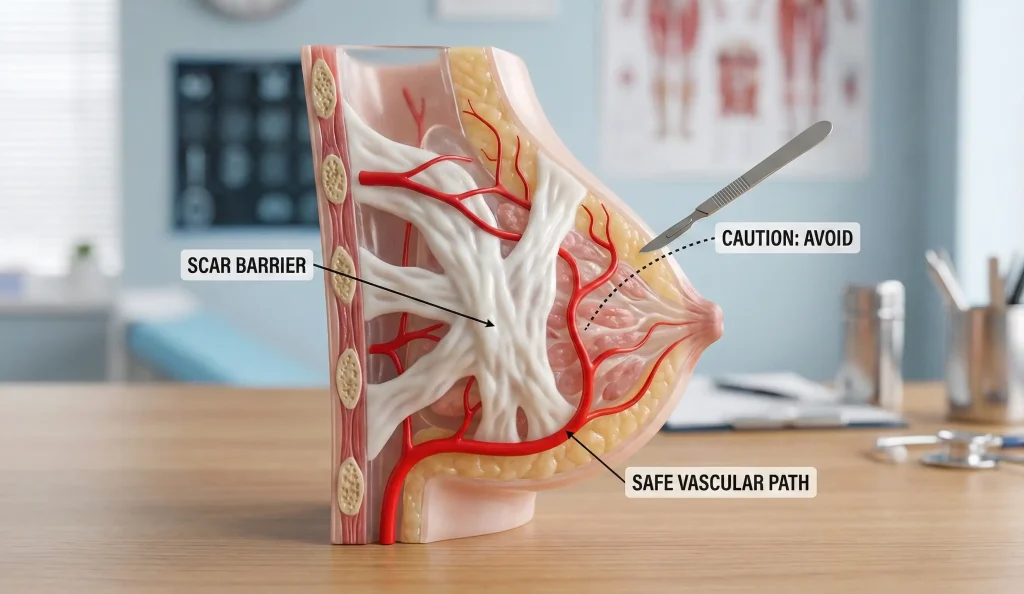
One of the main issues that make the doctors decline performing a second breast reduction in most cases is the blood supply consideration. A virgin breast that has not undergone any surgery previously, has a very good and fairly stable blood supply to the nipple-areola complex (NAC), coming from the internal mammary and intercostal arteries through deep branches. During your first breast reduction, the surgeon picked a specific “pedicle”—a piece of tissue carrying blood vessels to the nipple—and cut away the surrounding tissue. This changed the vascular pattern of your breast permanently.
When the second operation is performed, the surgeon has to work around scar tissue. Often, we are unaware of the exact pedicle that was utilized by the previous surgeon and we have no clue as to the strength of the remaining blood vessels. The easiest way to understand the problem is to imagine that we want to lift the nipple on a new pedicle that crosses the old scars which means that our only blood vessel is the one we will sever by cutting that pedicle. Nipple necrosis (partial or total death of the nipple and areola) can be the result. To lessen the chance of this, we might have to perform an MRI or obtain the previous surgery’s detailed operative notes in order to figure out blood flow even before the initial incision is made. In fact, a safe second breast reduction is to be interpreted as being mindful of the restrictions of the tissue’s endurance, not just the patient’s desire to continue removing.
Free Nipple Graft: A Safe Haven
When the patient wants the breasts to be significantly reduced (e.g., from a D cup to a B cup) or if the nipples are to be relocated very far upwards, the blood supply may be so unreliable that a standard technique with a pedicle would be too risky. In cases like these, the safest way to perform a second breast reduction might be through a free nipple graft (FNG).
The procedure includes taking out the nipple and areola completely from the breast—cutting all nerve and blood connections—and then surgically trimming the breast tissue very aggressively. After the formation of the new, smaller breast mound, the nipple is reattached to the skin in the same manner as a skin graft. This method may sound extreme; however, it effectively removes the possibility of nipple necrosis because the nipple gets its nutrients and oxygen from the underlying wound bed (imbibition) instead of relying on a long, delicate blood vessel. With a free nipple graft, you lose permanently the nipple protrusion, sensation, and the ability to breastfeed. Nevertheless, for women with severe macromastia relapse, the compromise is often acceptable for the safety and size reduction assurance.
Liposuction-Only Reduction: The Minimalist Approach
Not every relapse will require a scalpel. Patients will be allowed to keep their breasts after the first surgery if their “regrowth” is mostly fat which is the result of weight gain or menopause and they don’t have significant skin laxity. In these situations, it might be possible to do a liposuction-only breast reduction, which is a much less invasive option for a second breast reduction.
In combination with technologies like VASER Liposuction, we can liquefy the fat and extract large amounts of fat through very small incisions of only 3mm without having to break the old anchor scars and without risking the blood supply of the nipple. Besides that, VASER has a mild skin-tightening effect. This technique is fitting for a patient who likes the shape and lift of the breasts but is just bothered by their heaviness or fullness. The vascular risk avoidance is complete and a fast recovery is offered. Nevertheless, it can’t raise the sagging breast or correct a low-positioned nipple. It is only a debulking tool which means that it is strictly meant for removal of excess tissue.
Lin Health Europe Clinic: The Superomedial Redo
Revision surgery at Lin Health Europe Clinic is seen principally as a reconstructive challenge. We prefer the superomedial pedicle technique if and when an open
Second breast reduction has to be performed. This particular method is highly regarded for its excellent blood supply coming from two separate sources, making it a safer choice for secondary surgery than the inferior pedicle techniques of the past.
Besides, a lot of the time, the surgery is coupled with chest wall liposuction on the side to get rid of those “side-boobs” recurrences of previous surgeries patients almost always complain about. By changing the breast’s footprint instead of merely lowering the projection, we are creating a youthful, bouncy contour that defies gravity. Post-operatively, we are not shy in recommending Hyperbaric Oxygen Therapy (HBOT) at least for the revision patients as oxygen-rich blood goes a long way in helping the healing of scar tissues and it also supports the compromised nipple viability.
Frequently Asked Questions About Second Breast Reduction
It has been a higher-risk event than the first, especially in terms of wound healing and blood supply to the nipple. Nevertheless, in the scenario of a skilled surgeon with the correct technique (usually Free Nipple Graft), a second breast reduction is a safe and efficient operation.
The danger is considerably greater for a secondary surgery. When a free nipple graft is performed, the loss of sensation is permanent. With a conventional pedicle, the sensation may be reduced as a result of scar tissue interference.
Practically speaking, it would be extremely unlikely. One of the effects of the first operation that is likely to have been the cutting of some milk ducts; the second breast reduction generally will disconnect completely the remaining ducts, which is especially the case if a substantial amount of tissue is removed.
Usually, we require our patients to wait at least a year after their first surgery. It is that time required for the scar tissue to mature and become soft, as well as for the blood supply to stabilize before the second breast reduction is done.
Among the top reasons for a patient to come back for a second breast reduction are sufficient weight gain, pregnancy, or hormonal changes (e.g., menopause) that alter the fat-gland ratio of the breast.
Hamdi, M., et al. (2005). Secondary reduction mammaplasty: risks and benefits. Plastic and Reconstructive Surgery.
Abboud, M., & Vadoud-Seyedi, J. (2010). Revision of breast reduction: A 10-year experience. Aesthetic Plastic Surgery.
Spear, S. L., et al. (2012). Recurrence of macromastia after reduction mammaplasty. Plastic and Reconstructive Surgery.
Moufarrege, R. (2020). The concept of the ‘vascular supercharge’ in secondary breast reduction. Aesthetic Surgery Journal.