
Yes, minor surgery can correct inverted nipples.
Millions of women and men are deeply and silently insecure about the way their nipples look. Society is obsessed with the size and shape of breasts, but rarely talks about nipple-areola complex, which remains a secret shame. Women suffering from inverted nipple condition keep their feelings to themselves most of the time and even stay away from intimate life, using communal changing rooms or wearing tight clothes. The condition, medically referred to as an inverted nipple, is not an illness or an indication of poor health but simply one’s congenital anatomical variation.
The query, “Can you fix an inverted nipple?”, is one of the frequently asked questions that we at Lin Health Europe Clinic hear, but usually, the patients ask it quite quietly. The response is that inverted nipple surgery is a highly efficient, very minimally invasive procedure which can restore the projection of the nipple permanently. Nevertheless, one should be well aware of the details of the anatomy i.e. the lactiferous ducts when making a decision. Also, the surgical procedure used is dependent on the severity level of the inversion. We see it as our role to educate our patients on medical facts so that the topic can be shifted from a problem to a solution.
Understanding Inverted Nipple: The Short Duct Theory
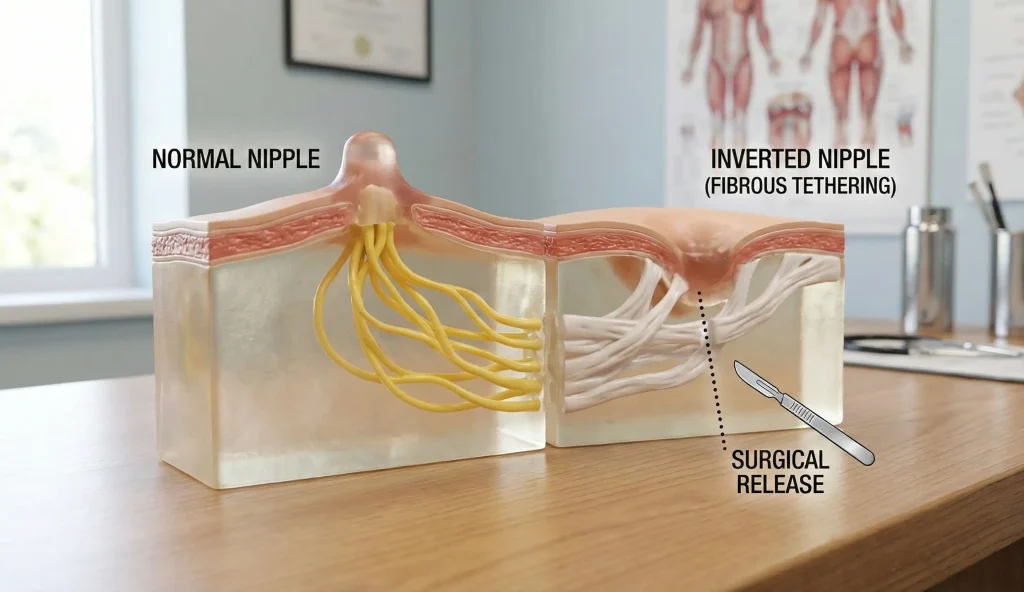
To find the etiquette of an inverted nipple, the first thing that has to be done is to know how the nipple is off a surface. It’s not just skin, but multiple ducts from the inside of a breast go right through a nipple, through 15 – 20 milk ducts (lactiferous ducts). These ducts have highly dense bands of fibrous connective tissue surrounding them, which are called collagenous tethers.
In a normal nipple, there is enough length for these ducts to extend beyond the surface of the areola. Genetically, the milk ducts are too short or the fibrous bands are too tight when someone has an inverted nipple. So in that case, those fibrous bands restrain the nipple’s outward movement mechanically, thus pulling it toward the chest wall. No hand pulling or suction device can elongate these biological tethers forever however, only surgery can release the tension. Therefore, the “fix” is mechanical: we must release the tether that is holding the nipple hostage.
The Grading System: Not All Inversions Are Equal
A major part of the planning of a surgery is determining the severity of the inversion based on the Han and Cheon Grading System. The diagnosis of this is a key factor to be able to save the milk duct.
Grade 1 inversion is kind of a “shy” nipple that due to manual stimulation or cold exposure becomes out for some time. This means that the ducts have some flexibility. Grade 2 inversion is the nipple that can be pulled out but once the pressure is released it goes back immediately. Grade 3 inversion, on the other hand, is so severe that the nipple is deeply embedded and can not be pulled out at all; it usually looks like a slit or a dimple. Grade 3 inversions are very often infections cases due to picking up on the bacteria trapped in the fold. In the case of Grade 3, surgery is done not only for cosmetic reasons but also for prevention of chronic mastitis which is a medical necessity.
The Surgical Solution: Lactiferous Duct Release
The best choice for a permanent correction is a microsurgical duct release. Usually, the operation is done with local anesthesia, so that the patient remains conscious, only numb, and it lasts no longer than an hour.
The surgeon cuts a very small incision – less than 5 millimeters in most cases – at the base of the nipple. Following this tiny hole, the surgeon identifies the tight fibrous bands that are endangering the ducts. For Grade 3 cases, the severed portion of the duct must be from the point of the most recent incision. After the release, the nipple will move forward in a natural manner. To keep the nipple from becoming retracted during the healing period, we use an internal “purse-string” stitch that works like a scaffold or a belt holding it in its newly corrected, projected position. This variation is structural and physical, which can resist the pull of gravity and scar tissue.
The Breastfeeding Dilemma: Function vs. Form
During the inverted nipple surgery, the most important thing discussed is the ability to breastfeed in the future. That is where the distinction between “saving” and “cutting” of the ducts becomes essential.
If the inversion is Grade 1 or mild Grade 2, the duct-sparing technique can be used. The fibrous bands around the milk ducts are released by the surgeon, the ducts themselves are not damaged. The capability to breastfeed is preserved, nevertheless, there is a somewhat bigger risk that the nipple might invert again. However, it is the ducts themselves that are the problem in Grade 3 cases. They are so short that they cannot ever work correctly. In this situation, the ducts must be completely cut to obtain the desired cosmetic effect. It is made clear to the patient that this Complete duct release means no breastfeeding from that breast. For most women with very severe inversion, who anatomically wouldn’t have been able to breastfeed anyway, it is a very reasonable sacrifice for having a normal look and hygiene.
Recovery and Sensation: What to Expect
It is hard to believe that the healing process after an inverted nipple correction operation can be quite fast. Usually, the majority of patients come back to their work the very next day. The main point is that the nipple must be left uncompressed to stay in the fully extended position during the healing process. For this purpose, a special stent or a “donut” dressing is used for a period of about 5 to 7 days.
Many of the patients feel scared about the loss of sensation. Most probably, patients with severe inversion already have very little or no sensation at all since the nipple is hidden. After the operation, the sensation is usually difficult to predict completely. Due to the local anesthesia and dissecting, some patients feel numb temporarily, while others keenly feel that their nipples are rubbing against the sleeves of their clothes. It is very likely that normal sensation will be restored within the timeline of 3 months, as the nerve endings will have healed. However, the psychological effect is immediate. Usually, when people see their projecting nipples for the very first time, their emotional state will jump, body image and sexual confidence are positively affected.
Frequently Asked Questions About Inverted Nipple Surgery
Since the operation is conducted under local anesthesia, there is no pain felt during the surgery. After, patients generally describe the feeling as a mild discomfort or slight tingling akin to a scrape that can be easily relieved with standard pain medications.
In case you decide to go for the total duct release method to ensure nipple projection, breastfeeding will not be possible. If we take a duct-sparing approach, it might still be possible to breastfeed, although it is not a guarantee.
While nipple piercing could physically help an inverted nipple of Grade 1 to protrude, it cannot repair the fundamental problem of the short milk ducts. If the piercing is taken out, the nipple will typically retract again. The only lasting way to resolve the issue is through surgery.
There are some instances where insurance can cover the cost. For example, if inversion is causing continuous infections, rashes, trouble breastfeeding (functional impairment) among other issues, the insurance company may pay for the correction. Cases that are only for cosmetic purposes usually have to be paid by the patient.
Relapse is uncommon with the duct release method utilized for Grade 3 inversions. But, after preserving the ducts to maintain breastfeeding, there is a slight increase in the risk (around 10-15%) that the nipple may become retracted again in the future.
Han, S., & Hong, Y. G. (1999). The inverted nipple: its grading and surgical correction. Plastic and Reconstructive Surgery.
Hernandez-Richter, T., et al. (2004). Surgical correction of the inverted nipple. Aesthetic Plastic Surgery.
Olivas-Menayo, J., & Berniz, C. (2020). Inverted Nipple Correction: Techniques and Outcomes. Aesthetic Surgery Journal.




