No, gynecomastia is gland tissue, not fat.
Men’s chests are, for a lot of them, a great source of worry. Instead of the cliché six-pack abs or pectoral muscles, they see a chest that is soft, protruding, and with a female outline. The situation has impacted the lives of millions of men globally and has been a major factor in their refusal to be seen in a swimming pool, their hunching of shoulders, or their wearing of double-layered shirts even in hot summer to hide their figures.
One of the biggest confusions is in diagnosing the condition. Is it just a case of excess body fat or is it an illness? The latter refers to a situation where a gym membership would solve the problem while the former points to surgery as the only solution. Medically, they are two totally different conditions: True Gynecomastia (enlargement of the glandular tissue) and Pseudogynecomastia (larger volume of fat). Knowing the difference is very crucial because a gland cannot be “burned” no matter how hard one diets. Lin Europe Clinic is a clinic male chest contouring oriented which daily decides for their patients what can be exercised away and what has to be surgically removed.
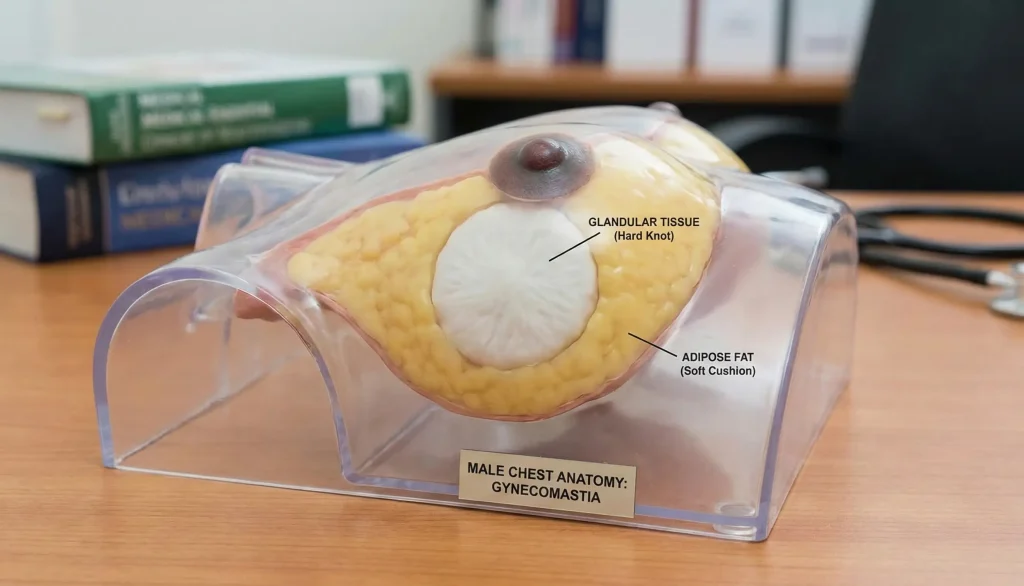
The Biological Difference: Gland vs. Fat
You need to examine what is underneath the skin if you want to understand why your chest is as it is.
- Pseudogynecomastia (Chest Fat): It involves only fat stored in the chest area. The fat is similar to that which is found in the stomach or thighs. It is soft and spongy as well as even inconsistency. Generally, it goes hand in hand with being overweight or a high percentage of body fat, heredity can lead to thin men storing fat in this way too.
- True Gynecomastia (Glandular Breast Tissue): This is the breast gland itself that is increased in size. It might sound odd but men do have glandular breast tissue and it can increase in size. The tissue is hard, fibrous, and rubbery. Imbalance of hormones (high level of estrogen or low level of testosterone), taking anabolic steroids, certain medications, or pubertal development are some of the causes.
The “Pinch Test”: How to Feel the Difference

Although only a medical practitioner can make a final diagnosis, you may, in many cases, at your home differentiate them by doing the Pinch Test.
Take a position flat on your back and put your thumb and index finger on both sides of your nipple.
- If it is soft: If there is only fat in the area with a soft texture and fingers meeting easily with only a soft, yielding resistance that is very much like the fat on your belly, then it is probably pseudogynecomastia.
- If there is a rubbery disc: If a firm, rubbery, or hard lump is felt directly behind the nipple – it is often likened to the texture of gummy candy or a grape – that is True Gynecomastia. The lump may or may not be tender, and it might be sensitive to the touch.
- The Combination Type: Most probably, it is a blended type. Glandular tissue surrounded by excessive fat is typical of men.
Here’s why gym is not the solution but the problem Very Often
It is a pity that the man who tries at the gym for years to make “bench presses” and gets rid of his gynecomastia is the man who eventually finds out that it does not leave. He sheds the pounds and develops huge chest muscles only to realize that his nipples protrude even more than they did prior to the commencement of the exercise program.
The reason is that the gland is not something you can “burn”. It is fuel that the body cannot break down for its energy needs since glandular tissue is one of them. Fat loss results in the disappearance of the fat around the gland, but the gland retains. Besides that, the pectoral muscle that is built behind the gland lifts the gland further thus making it more visible. If your body fat is low (with abs showing) but you still have nipples that are puffy, then you have true gynecomastia and the single solution for its removal is surgery.
The Treatment: Lipo vs. Excision
Since the tissues differ, so too do the surgical instruments used to remove them.
- Liposuction (For Fat): VASER or High-Definition Liposuction can, if you have only Pseudogynecomastia, be the solution. First, we break down the fat and then draw it out through tiny and imperceptible cuts. The immediate result is the flattening of the area.
- Surgical Excision (For Gland): Liposuction fails to extract glandular tissue that is hard because it is too fibrous. Excision is necessary. A small and inconspicuous cut is made by the surgeon at the edge of the areola (the point where the darker skin meets the lighter skin) and the gland is physically removed.
- The Duo: At Lin Europe Clinic, for the majority of our clients, we go for the mixed method. Contouring of the chest and blending of its edges is achieved through liposuction and a small excision is performed to remove the rubbery button of gland behind the nipple.
Hormones and Steroids: The Root Cause
Basically, True gynecomastia is a hormone disorder. Many boys get temporary breast buds at a certain period during their development when estrogen and testosterone hormone level changes. Most boys’ breast buds disappear within a short period of time, but for some, they persist.
Use of Anabolic Steroids is an aggravating factor of gynecomastia in adults. When men introduce testosterone from outside into their body, part of this hormone is converted into estrogen (a process known as aromatization) which promotes breast tissue proliferation. Made up of hard, dense, and inelastic tissue, the gland is usually very fibrous for these patients. We recommend the cessation of steroid usage for patients who are planning to undergo surgery. If they continue, there is a risk that the removed gland will grow back.
Experience the Lin Europe Difference: Masculine Contouring
Instead of merely “taking out the lump,” the team at Lin Europe Clinic sculpts a male chest. A male chest is not without contour; it has muscular definition, a specific slope, and contour.
To bring out the shadow of the muscle, we utilize VASER Liposuction for pectoral border etching. A “crater” or depression behind the nipple can result from the excessive removal of the gland when the gland is taken out, so we are careful about it. Our aim is a smooth, athletic chest surface that looks perfectly natural, whether you are wearing a t-shirt or are shirtless at the beach. We are aware of the embarrassment caused by the condition and our staff is very discreet and provides support to help you regain your self-confidence.
Frequently Asked Questions About Gynecomastia vs. Fat
If it is a condition of Pseudogynecomastia (chest fat), wear loss will work to reduce it. However, if it is True Gynecomastia (gland), wear loss will get rid of the fat around but the rubbery gland under the nipple will be left.
There will be tiny (3-4mm) liposuction scars and they will be hidden in the armpit. To remove the gland it is necessary to make a small curved incision on the edge of the areola which heals so well that the scar blends in with the natural pigment change of the nipple.
In general, no. You can’t get the gland to grow again once it has been surgically removed. But if you gain a lot of weight (fat accumulation) or use anabolic steroids again, you can get full again.
No pills that you can buy at the store work. Sometimes prescription medications such as Tamoxifen can be used to reduce the painful acute swelling in early puberty, but it is rare that they can eliminate the fibrous glandular tissue that has been established in adults.
Definitely. One of the main purposes of the surgery is to get rid of the “puffy nipple” appearance. The areola will be flat against the chest instead of coming out in a cone shape.
Rohrich, R. J., et al. (2003). Gynecomastia: Classification, surgical technique, and analysis of 244 cases. Plastic and Reconstructive Surgery.
Handschin, A. E., et al. (2008). Surgical treatment of gynecomastia in the bodybuilding patient. Plastic and Reconstructive Surgery.
Waltham, M., et al. (2014). Standardisation of the definition and treatment of gynecomastia. Journal of Plastic, Reconstructive & Aesthetic Surgery.




