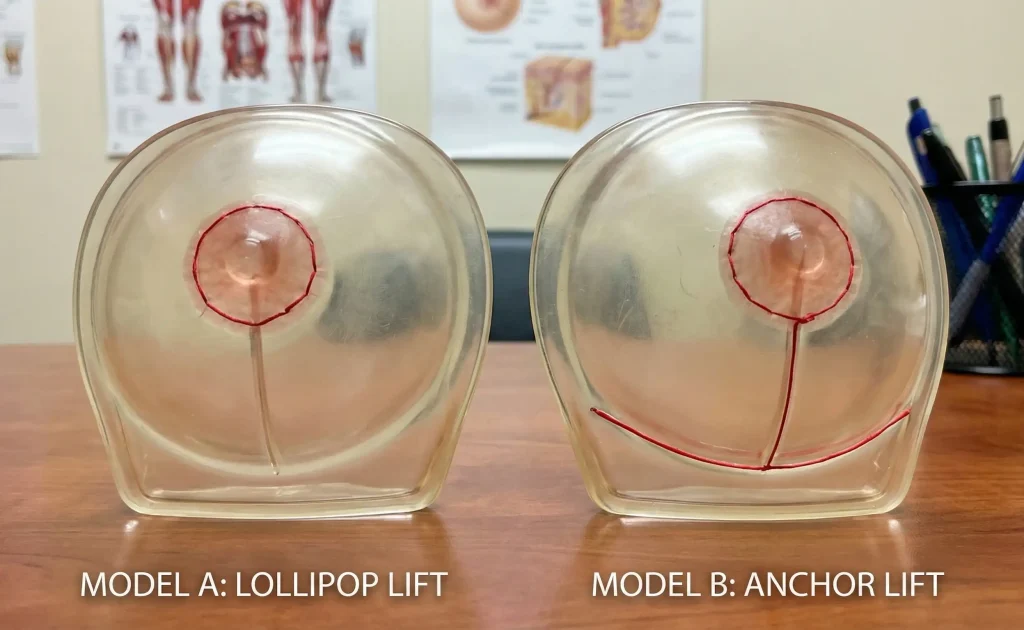
A lollipop lift has fewer incisions than an anchor lift.
When you first think about having a Breast Lift (Mastopexy), almost the biggest concern that usually comes up is the scarring. You want your breasts to look perky and youthful, but on the other hand, you really don’t want to exchange sagging skin for a network of scars that make you feel awkward when you are naked. This problem scares many patients and thus they go searching for the method that gives the minimum number of incisions. Eventually, such a search brings them to the debate between the two most popular surgical methods, namely the Lollipop Lift (Vertical) and the Anchor Lift (Inverted-T).
It is quite a common tendency among patients to consider the Lollipop lift to be “better” simply because there is one less scar. Nevertheless, plastic surgery involves a lot of geometry and trade-offs. Actually, the decision between these two methods is not only about the length of the scars; it has a lot to do with the amount of skin removed and the shape you want to end up with. At Lin Europe Clinic, we always insist on the technique which suits the breast rather than the breast having to fit the technique. Firstly, you need to figure out the differences between them mechanically so that you are ready to accept the scar, which will eventually give you the best outcome.
The Lollipop Lift (Vertical Mastopexy)

In fact, the word Lollipop Lift originates from the shape of the scar which is just like that of a lollipop: a circle around the areola (the candy) plus a single line vertically from the areola to the breast fold (the stick). There is no scar running horizontally beneath the breast.
The Ideal Candidate: This technique is most suitable for women with mild to moderate sagging (Grade 1 or 2 Ptosis) and good skin elasticity. It is perfect for cases where a patient needs a lift without having to drastically reduce the actual surface area of the skin cover.
The Mechanism: The surgeon makes an incision on the lower pole, pulls the edges together, and closes the incision.
The “Boxy” Phase: The Lollipop lift has a very interesting characteristic in that it has to undergo the healing phase. Since the surgeon gathers a lot of skin into a vertical line without a horizontal release, the bottom of the breast might look wrinkled, pleated, or slightly “boxy” after the operation. You have to be a little bit patient, as the skin first usually clears up and then rounds to a natural curve within 3 to 6 months.
The Anchor Lift (Inverted-T Mastopexy)
The Anchor Lift is the time-honored standard of breast surgery. The scar pattern in this case represents a complete circle around the areola, a vertical line down the center, and another horizontal line hidden in the inframammary fold (the crease under the breast).
The Ideal Candidate: This method is the only option for women with very severe sagging (Grade 3 Ptosis), patients after major weight loss, or those with very inelastic, “over-stretched” skin. If your nipple is pointing down or it is located considerably below your breast fold, you are most likely to require an anchor lift.
The Shaping Power: Having a horizontal incision enables the surgeon to dress a huge amount of redundant skin from both vertical and horizontal directions. This means that the surgeon has better control over the 3D shape of the breast, can constrict the breast footprint, and can produce a very tight, round, and projected mound that no Lollipop lift can produce on a heavy breast.
The Trade-Off: Shape vs. Scar

The basic difference is that it pertains to the Geometry of Reshaping.
Imagine wrapping a spherical gift. When there is too much paper (skin), then taping it in one direction will not be enough; at the bottom, you will be forced to fold it in order to make it fit the box tightly.
If you try a Lollipop lift on a breast that requires an Anchor, you will have a “bottom-heavy” breast in the end. As you chose not to remove the horizontal excess skin, the breast might appear to be long or wide at the bottom, hence the lack of a tight, perky round shape. The nipple could be up, but the shape will not have that tight, youthful curve. If you take the Anchor scar, you would have the shapeliness. Even though the scar is longer, the horizontal part is normally pretty well camouflaged in the natural shadow of the breast crease. It maybe is a quite thin white line hidden in the fold for most patients to be an ok trade for a perfectly round, high breast profile.
Longevity: Which Is a More Lasting One?
The surgeons are divided about which therapy would more effectively resist the inevitable pull of gravity. Roughly speaking, the Anchor Lift is thought to be the one which stays longer for the ladies with heavy breasts. By taking skin in two directions (up and down as well as side to side), the surgeon makes a skin envelope that is, in a sense, “tighter” thus a better “internal bra.”
The Lollipop lift heavily counts on the skin’s quality to be able to contract and snap tightly around the breast. If the tissue is bad (e.g., thin, sun-damaged, or post-bariatric), some Lollipop lifts will be faster in “bottoming out”, meaning that the breast tissue slides down the chest wall and settles into the bottom of the skin sack again within a few years.
Surgical Expertise in Turkey
At Lin Europe Clinic in Turkey, scar management is our specialty. We know that the “Anchor” seems like a nightmare but our techniques in suturing are meant to make it as invisible as possible. We perform layered closure techniques by separately stitching the deep tissue, the dermis, and the outer skin. Tension is what causes wide, ugly scars; by removing the tension, we encourage the scar to heal as a fine, hairline mark.
It is not just a guess, but a simulation of the lift during your consultation. We will actually show using your own body why a Lollipop can give you “dog ears” (excess puckered skin) at the ends of the scar, and why an Anchor can also mean a smoother, more aesthetically pleasing contour despite the extra centimeters of incision.
Frequently Asked Questions About Lift Techniques
Not really. Although there is less length of the incision, there can be a higher tension on the vertical line which leads to the “pleated” skin needing to settle time before it gets flattened and usually slows the healing process.
No, not if the horizontal part of the anchor scar is situated just right in the inframammary fold (the crease where the breast meets the ribcage), it will be hidden entirely even by the smallest bikini top or bra.
It is the appearance of “bossing” or bundling mainly along the vertical incision center that is intended and almost always disappears up to around 3 to 4 months after surgery when the skin becomes more relaxed and smooth.
Risk of loss of nipple sensation is more or less the same in both techniques because it depends more on the “pedicle” (the patch of tissue that supplies blood and nerves to the nipple) than on the skin incision pattern.
Absolutely. In case you undergo a Lollipop lift and are dissatisfied with the “bottoming out” or leftover loose skin, then it is possible to have a revision surgery that changes the former into an Anchor lift to further tighten the lower pole.
Lejour, M. (1994). Vertical mammaplasty and liposuction of the breast. Plastic and Reconstructive Surgery.
Hammond, D. C. (1999). Short scar periareolar inferior pedicle reduction mammaplasty. Plastic and Reconstructive Surgery.
Rohrich, R. J., et al. (2004). The spectrum of vertical mammaplasty. Plastic and Reconstructive Surgery.




