Usually one cup size increase per session.
For a lot of women, the idea of turning their extra body fat into breast enhancement is a winning scenario. It suggests that they can get a liposuction slimming effect in their stubborn areas like abdomen or thighs, at the same time, have a natural, soft breast augmentation that won’t carry any risk of implant rupture or capsular contracture. This procedure, medically termed as autologous fat grafting, is becoming increasingly popular as the “natural” replacement for silicone. Unfortunately, a lot of patients suffer the disappointment of encountering limits in volume that they had not anticipated. They dream of changing their cups from a tiny A to a full D in just one surgery, convinced that simply because they have a lot of fat in their body, they can relocate it all to their chest.
In fact, the results of a fat transfer breast augmentation are limited by the physiological principles of blood supply and tissue pressure. A fat graft, unlike an implant, which can provide a certain volume regardless of its pressure, is live tissue. It needs a healthy environment to continue living. If too much fat is packed into the breast, the graft will die. At Lin Health Europe Clinic, we are all about truthful communication and thorough information rather than just making sales. We intend to inform you of the exact biological limits of growth, the role of the “survival rate” of fat in determining your final result, and why the most important factor in this, multi-step treatment, is good timing.
One Cup Per Session Rule: The Reason Behind Volume Limits
The single most important measurement to be aware of in a fat transfer breast operation is the expansion limit. With a typical, single-session operation, you can’t realistically expect to go beyond half to one full cup size. Admittedly, this might seem slim compared to the instant switch of a 400cc implant; nevertheless, it is a substantial, permanent alteration of the breast in terms of its shape and fullness. The problem is seldom the quantity of fat that can be extracted but rather the recipient site—the breast—which is limited in its capacity to accommodate.
Your breast is made of a compact, tight bundle of skin and connective tissues. It only has a limited capacity. In case a surgeon puts 500cc of fat in a breast that physically can’t contain more than 250cc, the internal pressure (interstitial pressure) will shoot up. Such pressure leads to a collapse of the fragile capillaries which are supposed to supply the new fat cells. Without blood flow, the newly transplanted fat cells become deprived of oxygen and will die within a few days. That is why, practically, the amount of fat that we can inject is the one that still keeps the tissue soft and has a good blood supply. For them, we are looking at an amount of about 250ml to 300ml each breast, after the recovery phase, which translates to 150ml to 200ml of visible volume increase.
The Life-and-Death Matter of the Fat: Neovascularization

Essentially, we perform a transplant when we take fat from your stomach and graft it into your breast. The grafted fat cells (adipocytes) die off and become dysfunctional due to lack of blood supply. After their injection, they have to survive for 48 to 72 hours by eating off (plasmatic imbibition) nutrients in the surrounding fluid until your body grows new blood vessels into them through the process called neovascularization.
Therefore, not the entire fat that you put in there makes it because of this frail biological period. Generally speaking, according to medical knowledge, the Retention Rate—the fraction of fat that manages to get a new blood supply and stay permanently—averages around 50% to 70%. So, if 300cc of fat is injected, your permanent increase in volume may only be 150cc to 180cc. Over a duration of 3 to 6 months, the remaining 30-50% of the injected fat is transformed into energy and naturally absorbed by your body’s immune system. This “shrinkage” is a feature of the process and is predictable. Thus, immediately after the operation, the breasts will be quite swollen and bigger than the final size as a result of both the swelling and the total volume injected; however, after 3 months, they will have shrunk to the final size. Patients need to understand and be prepared for this reduction in volume mentally.
Implications of Overfilling: Necrosis and Cysts
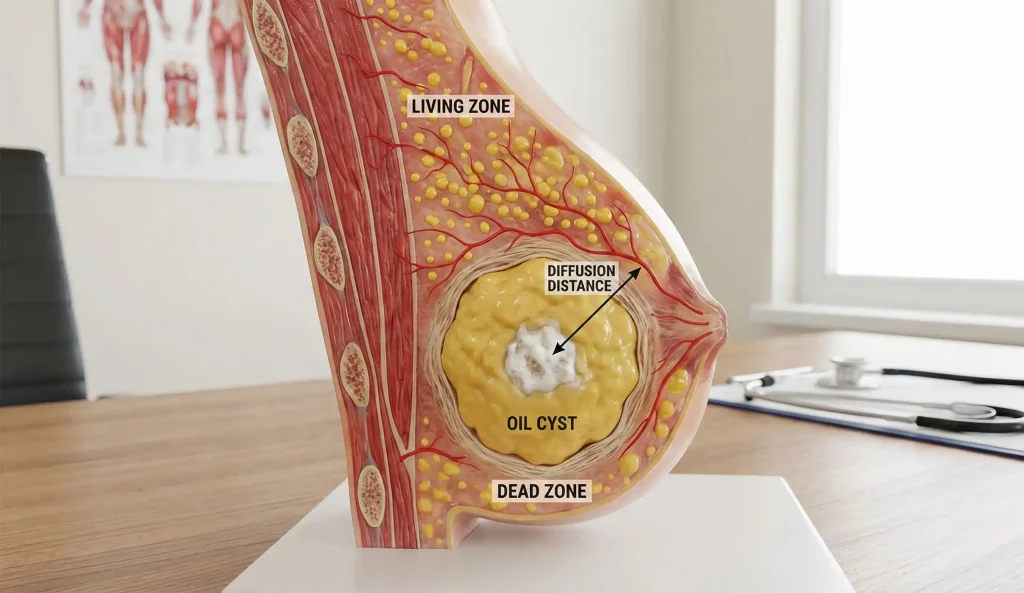
Someone may ask, “Why don’t we just compensate for the loss by overfilling the breasts?” plus the great A question a common follow-up to “why?”, but it’s a very risky and counterproductive method. Locally employing such a high-fat-concentration injection creates a “dead zone” in the middle of the graft which is deprived of blood vessels and therefore cannot receive any blood and nutrients. The central fat, which is the portion of the graft that is the farthest from the surrounding tissues and blood vessels, eventually dies, and this condition is commonly termed as fat necrosis.
Large regions of fat necrosis, which usually do not involve a single cell but rather a considerable number of them, can be quite problematic and, after a fairly prolonged period of time, can manifest themselves as painful lumps that have to be removed surgically. These lumps, medically known as Oil Cysts, can produce symptoms such as a burning sensation, pain or even swelling, and when they are confused with breast cancer tumors, they can cause patients to panic and anxiety, to the extent that a biopsy is necessary to exclude malignancy. In addition, the occurrence of numerous necrotic foci or lumps can increase the tissue’s susceptibility to infection and drainage problems. To prevent these problems, specialist surgeons at Lin Health Europe Clinic practice a method called distinct multi-planar layering that consists of injecting small quantities of fat into different layers of the breast—subcutaneous, intraglandular, and pre-pectoral—which ensures that every single fat cell is fit in the center of a healthy, blood-rich environment. This way, the fat survival rate is the highest, and the formation of hard nodules is minimized, yet we cannot add an unlimited volume in one session.
Donor Site Problem: “Spare Parts” Are Required

Your own anatomical makeup is another factor that limits the size increase of fat transfer breast. You cannot make your chest bigger unless you have enough of the rest of the body. For example, a very slender patient with a BMI of 19 who is after a C cup would basically be asking for something that is beyond her reach, because she simply does not have the raw material to assemble a house.
Generally, to obtain 600ml of highly purified fat (a quantity that will be sufficient for 300ml per breast), we will need to carry out liposuction on several regions of the body, such as the abdomen, flanks, thighs, and occasionally, arms. To eliminate the oil, blood and water, which results in further loss of volume, the extracted fat must be subjected to processing, filtering or centrifugation. In the event that a patient has very little body fat, we might only be able to extract enough to support a modest 100-150cc enhancement. Then, we will have an honest exchange of views on what the options are, one of which may be composite breast augmentation (implant plus a small amount of fat), to get the desired size without depending solely on donor tissue that is limited.
The Method of Multiple Sessions: Staging for Size
If the patient insists on using only fat to get a substantial size increase (for example, changing from an A cup to a C cup), then the safest way to do this is through serial fat grafting, where two or even three separate surgeries are performed, with at least 6 months‘ interval between each.
When the first operation is made, a new layer of vascularized fat is created and the breast envelope is expanded. When this new layer has recovered and softened (usually after 6 months), the blood supply will be stronger and the breast skin will be more stretchable. Therefore, the second round of fat can be planted in the second session on a “soil” that is now quite fertile. There can be an injection of another 250-300cc during the second session, which is an extension of the first session. Thanks to this gradual method, we can increase the volume to double without having the risk Factors that lead to necrosis or calcification. Extra time and funds are required, but this is the only method by which high volume with autologous tissue can be achieved.
Frequently Asked Questions About Fat Transfer Breast Size
On average, a permanent increase of anywhere from half a cup to a full cup size is what most patients can expect per surgical session. Trying to gain more almost always results in the death of fat cells.
Actually, the fat cells that survive the transfer (usually 50-70% of what is injected) form a permanent blood supply and function like normal fat tissue for the rest of your life.
This is very unlikely to happen with one surgery. To get that level of volume safely, you would likely need to have 2 or 3 separate fat transfer procedures, each spaced 6 months apart.
The fat that has been transferred is going to act very similarly to the fat in your belly. So, if you lose a lot of weight, your breasts will become smaller. If you put on weight, they will get larger.
At the time of the surgery, the breast is swollen and has fluid as well as dead fat cells. Within the first 3 to 6 months, the swelling goes down and the body takes back the non-surviving fat, thus revealing the real final size.
Spear, S. L., et al. (2014). Fat Injection to the Breast: Technique, Results, and Indications Based on 880 Procedures Over 6 Years. Plastic and Reconstructive Surgery.
Khouri, R. K., et al. (2012). Diffusion and perfusion: the key to fat grafting survival. Plastic and Reconstructive Surgery.
Delay, E., et al. (2009). Fat injection to the breast: technique, results, and indications based on 880 procedures over 6 years. Aesthetic Plastic Surgery.
Coleman, S. R., & Saboeiro, A. P. (2007). Fat grafting to the breast revisited: safety and efficacy. Plastic and Reconstructive Surgery.




